Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Obstetric Ultrasound
Your ultimate resource for Obstetric Ultrasound teaching files and Obstetric Ultrasound imaging & case of the day. Improve your diagnostic imaging skills online.
Posted in Obstetric Ultrasound on July 22, 2014 by m.khodeer
Chorioangioma Of Placenta
 
- A solid mass arises from the surface of the placenta, with considerable blood flow demonstrated on color Doppler
- Most cause no fetal problems, although fetal growth restriction and hydrops (from high-output CHF) may occur
Tags Chorioangioma Of Placenta
Posted in Obstetric Ultrasound on June 10, 2014 by m.khodeer
3rd trimester, screening US
 
ARPKD
- axial (Lt) and coronal (Rt) images of the fetal abdominal generate markedly enlarged echogenic kidneys, filling nearly the entire abdomen. Note also Oligohydramnios from decreased urine output.
- In severe cases, infant typically dies at birth from pulmonary hypoplasia; in less severe cases, hepatic fibrosis may cause death before renal failure
Tags ARPKD
Posted in Obstetric Ultrasound on May 20, 2014 by m.khodeer
(3rd trimester, screening US)

Holoprosencephaly
- Coronal image of the fetal brain shows the cerebral cortex (arrows) is fused across the midline and the falx is absent. Thalami are also partially fused
- Commonly associated with abnormal karyotype (often trisomy 13), as well as midline facial clefts, hypotelorism, and proboscis
Tags Holoprosencephaly
Posted in Obstetric Ultrasound on May 18, 2014 by m.khodeer
35-wk fetus
18-wk fetus
 
Answers
Hydrocephalus
- Axial view of a fetal head at 35 weeks gestation demonstrates a dilated lateral ventricle with + calipers measuring the width of atrium of lateral ventricle as 18.9 mm. the calipers are aligned perpendicular to the axis of the ventricle
- A 30-week fetus with dilated ventricles (+ calipers). Choroid plexus (arrowhead) is seen outlined by fluid [“drooping choroid”]
Causes of Prenatal Hydrocephalus
Aqueductal stenosis
Dandy-walker malformation
Chiari II
Communicating Hydrocephalus (e.g., prior hemorrhage)
Posted in Obstetric Ultrasound on May 12, 2014 by m.khodeer
Tags Tubo-ovarian Abscess
Posted in Obstetric Ultrasound on April 27, 2014 by m.khodeer
Posted in Obstetric Ultrasound on April 22, 2014 by m.khodeer
Hx of Polyhydramnios

Answers
Bowel Obstruction (Jejunal Atresia)
- Transverse view through the fetal abdomen reveals a dilated segment of bowel (arrowheads) filled with fluid and debris. Video clip demonstrated peristalsis within the dilated bowel loop
- The more proximal the obstruction, the more severe the polyhydramnios
Tags Jejunal Atresia, Bowel Obstruction
Posted in Obstetric Ultrasound on April 22, 2014 by m.khodeer
Multiple previous 2nd-trimester pregnancy losses
Different patient
 
Answers
Cervical Incompetence
 
- Image of the cervix in sagittal plane demonstrates spontaneous dilation of the cervical canal
- Second Image showed changing cervical length with transducer pressure
- Cervical length is the length of the closed cervix, normally >3 cm
Incompetent Cervix Stages

- Diagrams above show progressive funneling of the cervix: “Trust Your Ultrasound”
- Final stage is bulging membrances +/- fetal parts in vagina
Tags Cervical incompetence
Posted in Obstetric Ultrasound on April 10, 2014 by m.khodeer
Right Adnexa, + β-HCG
Representative image of Uterus
 
Tubal Ectopic Pregnancy
 
- Coronal transvaginal view of the right adnexa demonstrates an extauterine gestational sac (arrows) containing an embryo (calipers)
- Uterine cavity is empty
Good
Bad
 
- Left-An intrauterine gestational sac is surrounded by two echogenic rings, an inner ring (short arrows),and an outer ring (long arrows), corresponding to two layers of decidua ("double decidua sign")
- Right – sagittal transabdominal view of another patient demonstrates a fluid collection (arrows) in the uterus, with none of the characteristics of a gestational sac (no yolk sac or embryo within it, no double echogenic ring surrounding it). Such a fluid collection, representing blood or secretions in the uterine cavity in a patient with an ectopic pregnancy, has been termed a pseudogestational sac
Tags tubal ectopic pregnancy
Posted in Obstetric Ultrasound on April 08, 2014 by m.khodeer
AFI=37.5 cm
 
Polyhydramnios
- Images at 31 weeks gestation demonstrate subjectively increased amniotic fluid volume, due to a fetal neck mass that obstructed swallowing, on this sweep through the gravid uterus Deepest pocket measurements in the right upper quadrant (RUQ)
- Causes: Idiopathic (33%), Maternal Diabetes mellitus (25%), Multiple Gestations (10%), Fetal anomalies (20%), and Fetal hydrops (12%)
Tags Polyhydramnios
Posted in Obstetric Ultrasound on April 06, 2014 by m.khodeer
 
Conjoined Twins
- Transverse view through twin thoraces (S1, spine of twin 1; S2, spine of twin 2) demonstrates that they are joined anteriorly (arrows) and share a heart (arrowheads)
- Conjoined twins result from late splitting of a single fertilized egg, typically when the splitting occurs more than 12 days after conception. Various sited of union can occur, including:
Thoracopagus: joined at the thorax
Omphalopagus: joined at the anterior abdominal wall
Craniopagus: joined at the skull
Ischiopagus: joined at the pelvis – typically easier to separate
Tags Conjoined Twins
Posted in Obstetric Ultrasound on April 06, 2014 by m.khodeer
11 wks by LMP

Answers:
Multiple Gestations (Quintuplets)
  
Tags Quintuplets, Multiple Gestations
Posted in Obstetric Ultrasound on March 24, 2014 by m.khodeer
Vessel Umbilical Cord
- Axial image of the pelvis shows only 1 umbilical artery
- Color doppler shows only 2 vessels in the umbilical cord
- High association (50%) with other anomalies
- Sometimes, the cord has 2 arteries for part of its length; however, if there are 2 arteries at the fetus, it is considered normal
Posted in Obstetric Ultrasound on March 18, 2014 by m.khodeer

Answers:
Failed Pregnancy
 
- Left: Ultrasound video showed no heartbeat in an embryo with a crown-rump length > 5 mm, diagnostic of a failed pregnancy
- No heartbeat at a gestational age of 6.5 wks (if known with certainty) is also diagnostic
- Right – “Blighted Ovum”=Failed pregnancy: no visualized embryo with MSD > 16 mm is highlysuggestive of failed pregnancy (also referred to as “anembryonic pregnancy”)
Major Discriminators – can you recall?
- MSD > ? / ?* mm must have a yolk sac
- MSD > ? / ? Mm must have an embryo
- CRL > ? Mm must have a heartbeat (“Alive by ?”)
Major Discriminators – Repetition
- MSD > 10 /20* mm must have a yolk sac
- MSD > 18 / 25 mm must have an embryo
- CRL > 5 mm must have a hearbeat (“Alive by Five”)
Tags Failed pregnancy
Posted in Obstetric Ultrasound on March 05, 2014 by m.khodeer
Screening US.
Additional scanning gives the 4-chamber view above. Recommendations?

Additional Imaging
Real-time US of extremities.
Skull in a different plane than shown initially.
Choroid Plexus Cysts/ Trisomy 18

-Initial image demonstrated bilateral choroid plexus custs.
-These can be incidental, and do occur in 1.8-3.6% of normal fetuses, but…
-There is an association with Trisomy 18 (Edward’s Syndrome):
-In the absence of other abnormalities, 1/450 will have abnormal karyotype.
- In the presence of 1 other abnormality, 40 % have Trisomy 18 (=10x RR) (= additional defects 600 x relative risk!)
-Risk of fetal loss from amniocentesis is 1/250 Additional Images showed an AV canal, clenched hand, “strawberry” skull
  
OB Management of Choroid Plexus Cysts:
-Targeted search for additional anomalies: detailed evaluation of the heart, images of the face and feet, attempt to image the open fetal hand.
-If additional anomalies are found, amniocentesis should be offered
-If no additional anomalies are found, fetus is highly likely to be normal
Association with Trisomy-18:
-clenched hand with overlapping index fingers (highly characteristic), CHD, sever IUGR. MS-AFP, β-HCG, and Estiol are all low in Trisomy-18.
Related Information
-Difference between “lemon” and “strawberry” skull can be somewhat subtle, at best. -The “lemon” sign (as in Chairi ? malformation) seems to have more concave appearance to frontal bones
 
 
Tags trisomy 18, choroid Plexus Cysts
Posted in Obstetric Ultrasound on February 27, 2014 by m.khodeer
Amniotic Band Syndrome
 
- Lt: Sagittal image of a fetus demonstrates an intact head (H) and upper spine (arrow) and disruption of the anterior and inferior trunk. Abdominal contents (arrowheads) float freely within the amniotic cavity. The lower spine is absent.
- Rt: Membranes (arrowheads) are seen crossing the amniotic cavity adjacent to the fetal head (H).
Tags amniotic band syndrome
Posted in Obstetric Ultrasound on February 25, 2014 by m.khodeer
 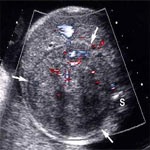
Left: There is a large heterogeneous solid renal mass (calipers), with only a small amount of normal renal tissue identified (arrows).
Right: Transverse views of the fetal abdomen demonstrate a large mass (arrows) in the expected location of a kidney, anterolateral to the spine (S).
Tags Mesoblastic Nephroma
Posted in Obstetric Ultrasound on February 23, 2014 by m.khodeer
12 wk fetus

Answers:
Oligohydramnios
Virtually no detectable amniotic fluid; the fetus died within 1 week of the sonogram
Remember “DRIPP”: Demise, Renal Anomalies, IUGR, Permature rupture of membrances, and Post-Dates
Tags Oligohydramnios
Posted in Obstetric Ultrasound on February 11, 2014 by m.khodeer
 
- Key finding above is that the folds (arrowheads) have a base which connects to the uterus, and a free edge. Color Doppler (right) shows blood flow in the majority of synechiae, which would be very uncommon for amniotic bands.
- Due to folding of amniotic membrane around synechiae, which are fibrous scars in the uterus (typically from prior instrumentation).
- Typically no complications: much better prognosis than amniotic bands.
Tags Synechia, Amniotic Sheet shelf
|




























































